

)
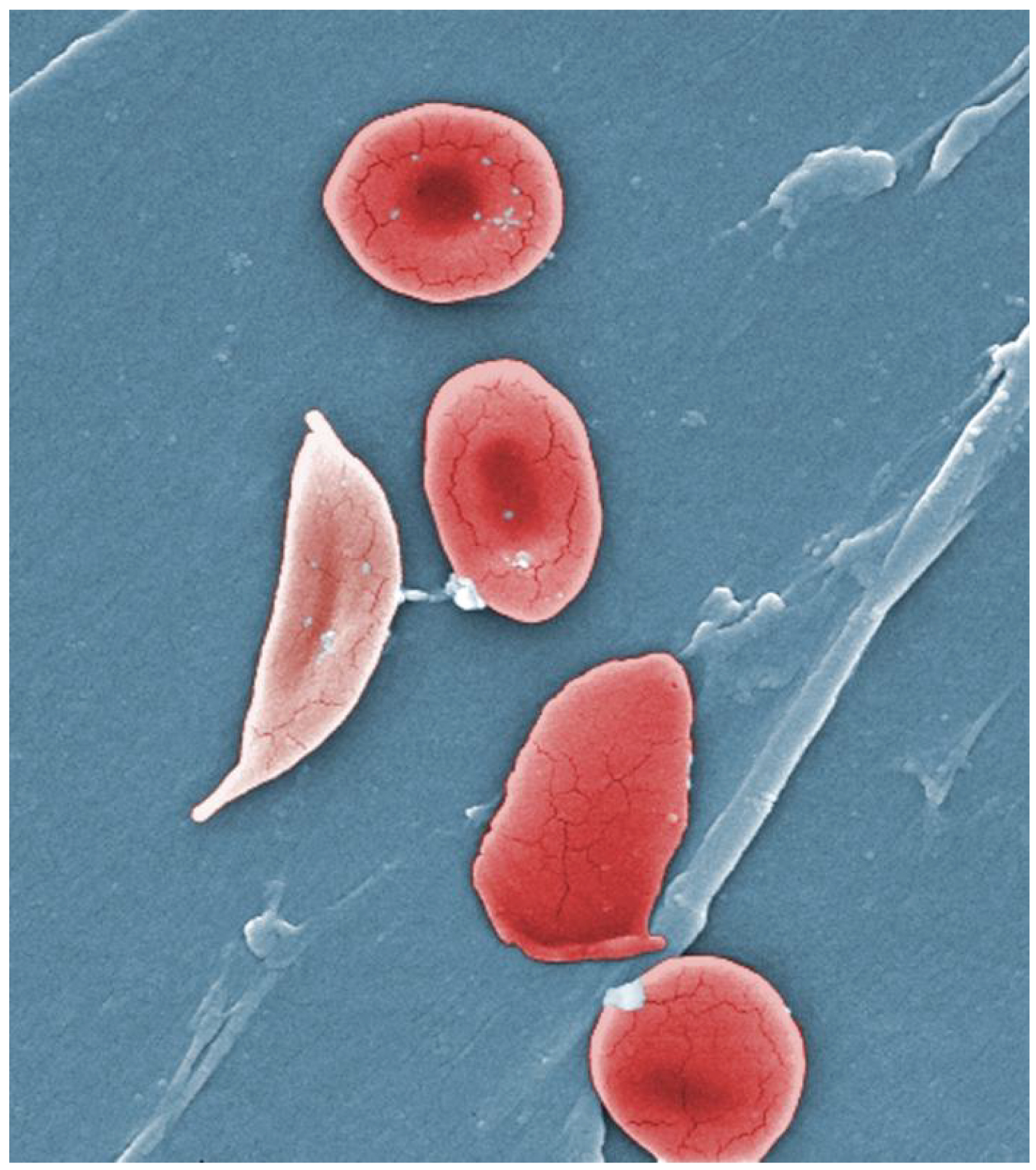
For all the expectant couple's pregnancy is a journey filled with anticipation, lifestyle changes, and a heightened focus on health. However, there are certain preexisting conditions in the expecting mother that pose serious health risks and challenges during pregnancy. One such condition is sickle cell anaemia. Sickle cell anaemia is a condition where in the affected individuals red blood cells crumple during times of stress and form the shape of a sickle. These cells are extra sticky and tend to block the minute blood vessels in the body leading to lack of blood supply to various organs. They also create an environment of increased inflammation in the body and cause the so called sickle crisis. During such an episode affected individual will experience severe pain in various parts of the body along with anaemia. They can have fever, breathlessness and in extreme conditions they may develop major complications like heart attack or stroke.
Globally around three lakh children are born with sickle cell disease. India has worlds second highest burden of disease for sickle cell anaemia. The prevalence rates reach roughly 1% with highest numbers recorded in Chhattisgarh, Madhya Pradesh, Gujarat and Maharashtra. Some pockets of Kerala and Karnataka also have increased sickle cell anaemia incidence. With advancement in treatment and supportive care measures, the sickle cell anaemia more children survive to adulthood. The incidence of girls with this disease growing healthy becoming pregnant also has increased proportionately.
The Intersection of Sickle Cell and Pregnancy
To understand why pregnancy impacts sickle cell anaemia, it helps to look at how the body changes when expecting. During pregnancy, a person's blood volume increases significantly to support the growing foetus, and the heart works harder to pump this extra blood. For someone with sickle cell anaemia, their red blood cells already have a shorter lifespan and can easily get stuck in small blood vessels, blocking blood flow. The natural stress and physical demands of pregnancy can increase the frequency of these blockages, leading to complications for both the parent and the baby.
Pregnancy in individuals with sickle cell disease (SCD) is a high-risk scenario that requires specialized, multidisciplinary care. While advancements in medicine have vastly improved outcomes, the combination of the physiological demands of pregnancy and the microvascular complications of SCD creates unique challenges for the parent, the foetus, and the management team.
Potential Risks For Mother And Child
Even with best of medical care the maternal mortality in sickle cell anaemia is six times higher than normal population. The anaemia is seen in all pregnant ladies with this disease. Almost all of these ladies need additional therapy for anaemia including iron supplementation and sometimes blood transfusions. Upto 60-90% of these patients will develop some form of sickle crisis during their pregnancy requiring urgent hospitalization. They also have increased risk of developing serious infections and needing antibiotics. Nearly one thirds of these patients will develop either asymptomatic bacteriuria, urinary tract infections or pneumonia. Development of placental insufficiency (reduced blood flow to placenta) is very common and as a result of this they are prone to develop increased incidence of preeclampsia (up to 10-14%) and hypertension during pregnancy. The risk of development of clot in the blood vessels also increases significantly in these patients. Lot of the patients develop preterm labour and need emergency C-section to safely deliver the baby. The preterm birth is 2.4 times commoner in this group of patients that normal population.
As far as the baby is concerned, there is increased risk of intrauterine growth restriction, premature birth and rates of in-utero death. If the mother was given opioid drugs like Morphine during pregnancy for long term, the baby may develop so called Neonatal Opioid Withdrawal Syndrome characterised by irritability, sleep disturbances, tremors. These babies will need prolonged hospital stay, many times increased neonatal ICU stay.
How to manage these patients?
Management requires an integrated team including a maternal-foetal medicine specialist (high-risk obstetrician), a hematologist, and specialized nursing staff. The delivery should happen in a hospital fully equipped with blood bank support and full-fledged ICU set up for both mother and child.
- Once lady with SCD becomes pregnant, her husband should undergo haemoglobin electrophoresis.
- If both parents carry a sickle gene, there is a 25% (1 in 4) chance the child will inherit SCD. Prenatal options include Chorionic Villus Sampling (CVS) at 10-12 weeks or amniocentesis at 15-18 weeks.
- If the child is found to have homozygous sickle cell anaemia, MTP can be done to safeguard both mother and to prevent lifelong suffering for the baby.
- If the child is normal, pregnancy can be continued depending of condition of the mother. Such ladies should get their blood tested every month and consult haematologist. The haemoglobin has to be maintained above 9-10gm%.
- If the patient has vaso-occlusive crisis, patient has to be hospitalized immediately and started on analgesics, oxygen and IV hydration. They may need blood transfusion if haemoglobin is less than 9gm%.
- For those who have Hb more than 9-10gm%, we may have to do exchange transfusion where we remove parts of the defective blood from the patient and replace with normal blood.
- Analgesics like NSAIDs are to be avoided in these patients because of increased risk of kidney injury.
- Patient will have to take blood thinners like aspirin and sometimes low molecular weight heparin injections regularly to prevent blockade of blood vessels and development of complications like pre-eclampsia.
- Foetal growth monitoring has to be done regularly and in case of IUGR, the patient may have to be transfused blood. Some drugs like Hydroxyurea may be given to these patients after 4th month of pregnancy to reduce the risk of sickle crisis and complications.
- These patients will need early initiation of antibiotics to prevent severe infections. Patients should be well hydrated and avoid strenuous activities.
With close monitoring, regular ultrasounds to track the baby's growth, and a dedicated healthcare team, the risks associated with sickle cell anaemia can be anticipated, managed, and minimized, paving the way for a joyful addition to the family. Every sickle cell anaemia pregnancy need to be considered as high risk pregnancy and has to be manged by team of specialist doctors.
(By Dr Prashanth B, Consultant Hematology, KMC Hospital, Mangalore)
Disclaimer: The opinions expressed within this article are the personal opinions of the author. NDTV is not responsible for the accuracy, completeness, suitability, or validity of any information on this article. All information is provided on an as-is basis. The information, facts or opinions appearing in the article do not reflect the views of NDTV and NDTV does not assume any responsibility or liability for the same.